
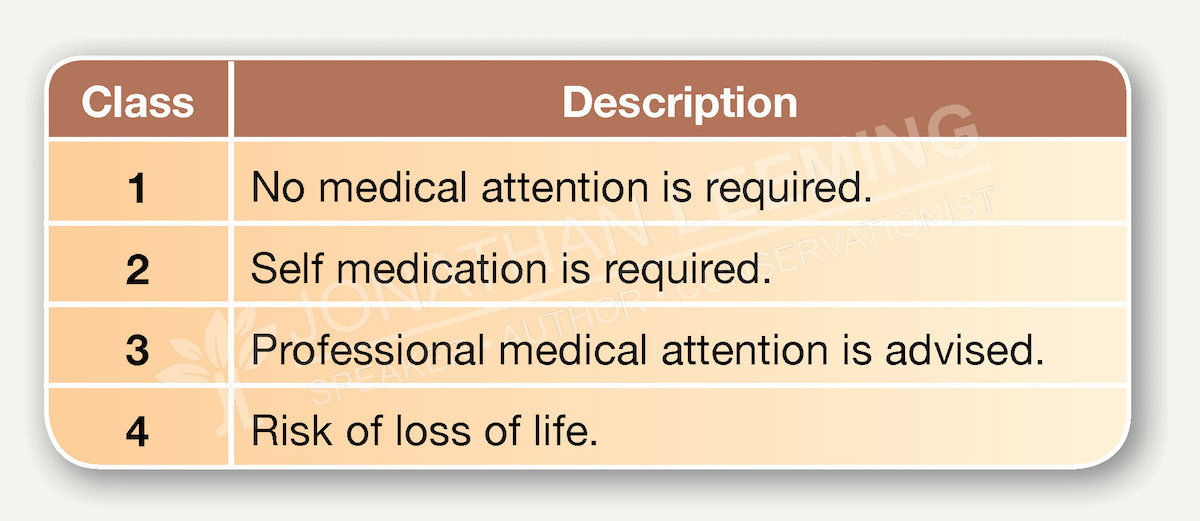
These classes also relate to bites and stings from other venomous animals, such as scorpions, snakes, stingrays, stone fish, centipedes, bees and wasps. These classes do not increase in equal steps nor on a linear scale, but rather define boundaries, indicate outcomes and required action. These classes relate to the sum of the patient’s symptoms.
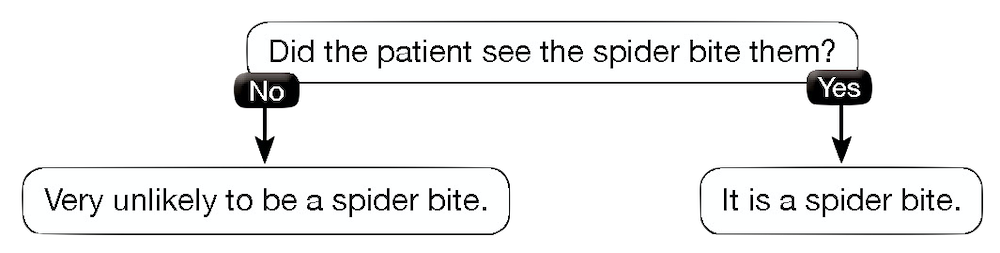
Spider bite symptoms can be divided into immediate and delayed symptoms. Recognising and understanding how symptoms develop is important for effective first response.
Understanding how symptoms develop and the associated timeframes, offer insight into the progression of symptoms from immediate to delayed.
The risk of bacterial infection is low because the bite site does not develop into an open lesion. Use of antihistamines is not advised unless the patient is experiencing an allergic reaction. Life threatening allergic reactions to spider venom are very rare.
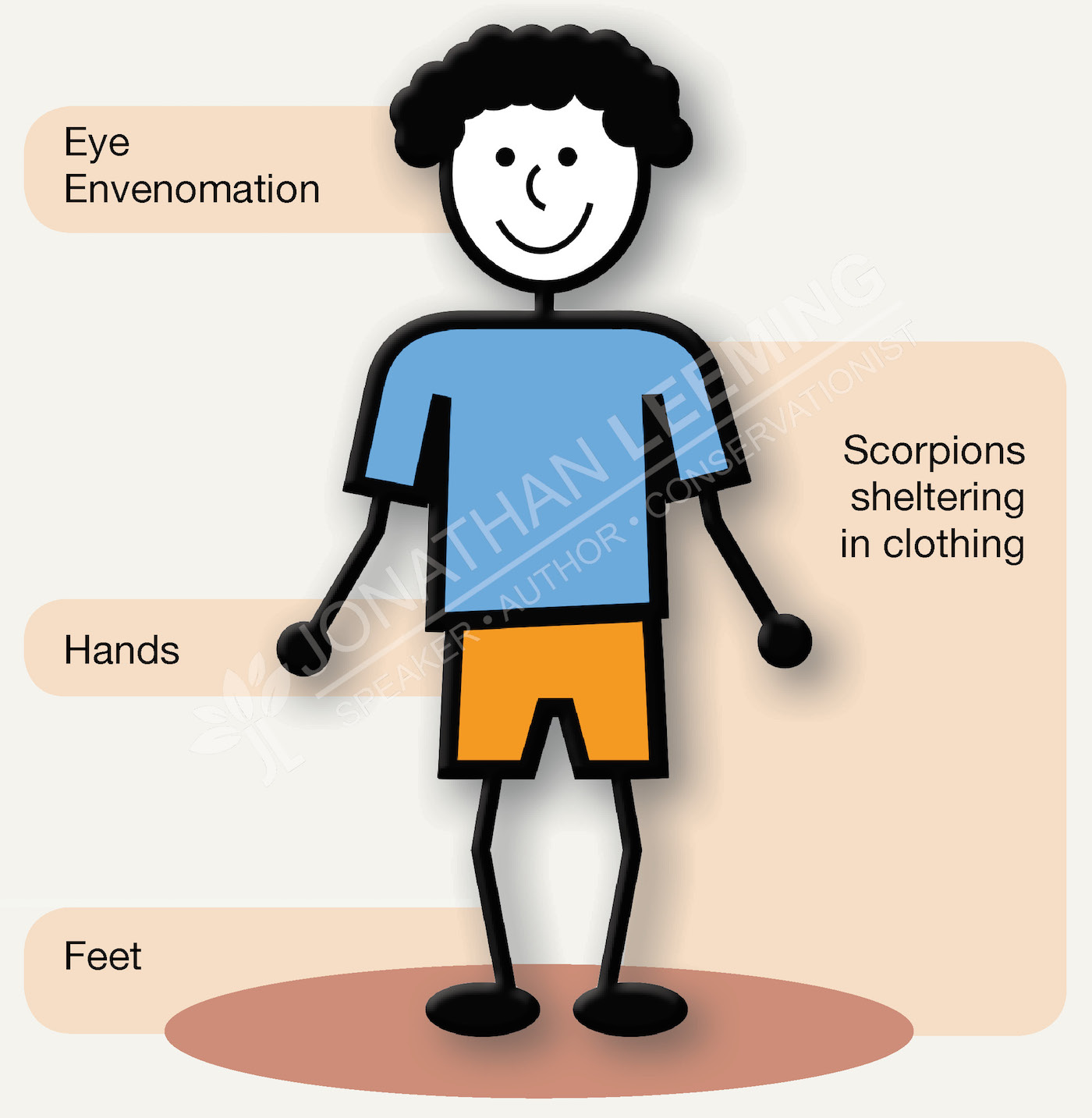
The majority of spider bites in humans occur when picking up objects under or in which a spider is sheltering, or when someone who is barefoot or is wearing open sandals stands on the spider. Animals are stung more often on the face, mouth or front feet.
Antivenom for the treatment of Southern African scorpion stings is manufactured by the South African Vaccine Producers (SAVP) at the National Health Laboratories in Johannesburg, South Africa.
An initial dose of 10ml (2 vials) is required intravenously, with an additional dose of 5ml (1 vial) every 6 hours until the symptoms improve. This additional dose is not always necessary. The same dose is used for children and adults. The effectiveness of antivenom is gradual, peaking between 2 and 6 hours after administration. SAVP scorpion antivenom is ineffective at treating a patient who has venom in the eyes. Allergic reactions to SAVP scorpion antivenom are uncommon or usually mild.

